VBAC The Ultimate And Comprehensive Q & A
VBAC The Ultimate And Comprehensive Q & A
By Nadia Raafat HBAC x 3 + VBAC doula
With the c-section rate escalating rapidly, (approximately 1 in 3 babies are born abdominally in the UK, in some trusts it’s 1 in 2 in April 2024) more and more women find themselves facing VBAC. Whilst there is still a lot of clinical anxiety around VBAC, for the mother there are many reasons why attempting VBAC brings much less long-term risk to her and her baby than another caesarean. Whilst the number of woman choosing VBAC remains low – just 13% in the UK. Of those that attempt VBAC, (according to the most recent national Audi 2023) there is a 61 per cent success rate. Disappointingly, this is 10 per cent down on previous figures which shows VBAC intervention is on the rise in line with general intervention.
This is nothing to do with your capacity; human bodies have not changed in the last 50 years; only hospital policy.
Whether you are considering VBAC/HBAC or have committed to your VBAC/HBAC or are supporting either, these questions and answers will prove an invaluable go-to resource for you. They are a mixture of questions raised at the recent live VBAC/HBAC session I recorded with my friend and mentor former independent midwife, most experienced birth educator and wise birth-keeper Joy Horner and myself – as well as additional questions I have received and come across during my VBAC research.
The VBAC/HBAC experience is a unique one that requires special knowledge and dedicated preparation. In choosing to VBAC or HBAC, we want to give ourselves every opportunity to complete the path we choose to walk – which must be necessarily a different path to the one we took on our previous birth as we are a different women navigating it.
I know. As I am an HBAC – three times over – and every time, my commitment has been seriously tested. I am deeply grateful for the lessons I have learned along the way.
1. Why Bother with a VBAC?
For many VBACs, the first birth was long and difficult; you may even have experienced birth trauma along the way. Dread is not an uncommon emotion for many women facing VBAC for the first time. You don’t necessarily trust your body; after all it may have appeared to fail you; perhaps you did not experience or certainly complete the second stage and you may well have felt disempowered and frightened along the way.
Attempting to birth again when it did not go to plan the first time, can feel huge; isn’t it easier just to bypass the whole experience with a second c-section?
Here’s are the advantages of a successful vaginal birth:
- A successful VBAC has the fewest complications. The absolute risk of birth-related perinatal death associated with VBAC is extremely low (4:10,000).
- VABC once and you have a much greater chance of a vaginal birth in future pregnancies. 85-90 % if you’ve birthed vaginally before. Whereas the more caesareans you have, the greater the long term risk to your body.
- An elective c-section brings greater risk to your baby; whose respiratory system can be compromised; whose bones forfeit the moulding of the birthing process; who’s physiology misses out on the cocktail of birthing hormones and whose microbiome suffers from early antibiotics. Babies derive immense benefits from vaginal birth.
- A deep sense of vindication and reclamation of your body when you succeed. This cannot be underestimated and informs the woman you become.
- Recovery and returning to everyday activities are likely to be quicker after vaginal birth. Being immobile is compromising, if you have a toddler or small child as well your baby to care for.
- By having a VBAC you avoid the risks of major abdominal surgery which include: an increased risk of placenta praevia/accreta and Pelvic adhesions which may complicate any future abdominal-pelvic surgery. There is also an increased risk of prolapse and pelvic floor issues.
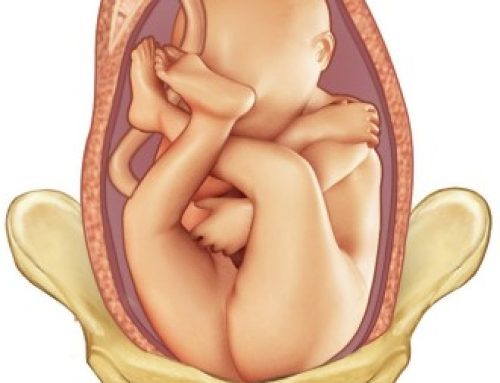
2. What is The Risk of my Scar Rupturing?
Scar rupture or scar dehiscence affects 0.2 women; that is around one in 200 women trying for a VBAC. Whilst that may seem significant, the absolute risk of birth-related perinatal death associated with VBAC is extremely low (4:10,000).
If induced, the risk increases to 2-3/200.
3. Are There Signs of Scar Rupture?
Yes. Most of the time. Although scar dehiscence can occasionally be silent.
These are the symptoms and signs of scar dehiscence/rupture which midwives are alerted to look out for:
- Vaginal bleeding.
- Uterine scar tenderness.
- Abdominal or referred Pain between contractions.
- Cessation of contractions.
- Pain “breaking through” epidural analgesia or excessive epidural requirements.
- Persistent CTG abnormalities (commonest finding).
- High Maternal Heart-Rate, hypotension, shock.
- Loss of station of the presenting part
- Blood in your urine
The presence of one of these symptoms/signs would alert the midwife to take appropriate action. The situation would almost certainly require hospital transfer if HBAC and the care of a consultant would be recommended.
4. What is the Difference between Rupture and Dehiscence?
Generally as in the above NHS document, the two categories are brought together. However this can be very misleading as dehiscence is not a medical emergency whereas rupture is.
The excellent us-based online resource www.VBACFacts.com offers a clear breakdown of the two.
“Uterine ruptures often presents with foetal heart rate abnormalities, haemorrhage, and/or abdominal or referred pain, particularly in the shoulder. Uterine ruptures can harm the foetus by diminishing, or eliminating, oxygen delivery which can result in brain damage or death. The primary risk to birthing women or people is excessive blood loss. As a result, uterine ruptures are medical emergencies even though not all uterine ruptures will result in an adverse outcome.” (VBAC FACTS)
A uterine dehiscence is when the myometrium (the middle layer of the uterine wall,) separates, but the serosa (This is the smooth outer layer which covers the uterus and makes it easy for the uterus to slide and move within the pelvis as needed.) stays intact. They can also be called a uterine window or an “incomplete” rupture.
“Dehiscence is often asymptomatic, does not require surgical repair, and is often only identified during a cesarean delivery or via ultrasound. Dehiscences typically do not pose any risk to the foetus or birthing parent. They are not medical emergencies.” (VBAC FACTS)
When reading medical studies, it’s critical to determine how a specific study defines uterine rupture. This is even more relevant when looking at more complicated scars like the Classical Scar or the T or J Scar.
For further info on VBAC with a classical scar please read this excellent resource:
https://vbacfacts.com/2021/08/10/uterine-rupture-classical-incision-vbac/
5. What Are The Risks of VBAC Besides Scar Rupture?
Short answer: the same as in any birth.
Much will depend on your obstetric history, the reasons for any previous caesarean(s), and whether you have previously given birth vaginally.
6. Who Should Not Attempt a VBAC?
There are very few women who, if they choose VBAC, should be advised against.The only absolute contradictions are previous uterine rupture or placenta preavia or similar.
If you have a breech baby and a uterine scar, multiple pregnancies or complicated uterine surgery, or if your scar is unusual, you will probably be cautioned against VBAC. If you have an unusual scar, like the classical scar, or T/J scar mentioned above, a VBAC will not be recommended however ultimately it is your right to choose. Scars differ, are situated differently and heal differently. Take an individualist approach to your scar rather than a blanket one. Always ask for a second opinion if you are not happy with the decision-making process.
7. Can I VBAC if I’m over 40? Or my pregnancy has lasted over 40 weeks?
Statistically speaking greater maternal height, maternal age less than 40 years, BMI less than 30, gestation of less than 40 weeks and infant birthweight less than 4 kg (or similar/lower birthweight than index caesarean delivery) are associated with an increased likelihood of successful VBAC. (Author: Sam Brabazon (ST3), D Nirmal (Consultant Obstetrician)
However, statistics do not recognise individual will, levels of coercion, degree of support or preparation, willingness to question and negotiate on matters of age, weight, gestation and bmi. I successfully VBAC-ed when my daughter was 42 weeks gestation. I successfully VBAC-ed my son aged 42.
Never deny yourself the opportunity to undertake a physiological birth because a guidelines based on statistics suggests you are not a good candidate. If a midwife or consultant recommends an induction simply because you are 40 years or 41 weeks – without any other risk factor – change your care provider.
8. What if my Baby is Big?
Clinicians are anxious about big babies. The policy is to not recommend VBAC if the baby weights more than 4000 grams: (8 pounds, 13 ounces.) However hold this information lightly as this recommendation is also widely contested within the birthing community. If you have a big baby, perhaps you also have a large pelvis; check your own birth weight, foot size to ascertain whether your baby is truly large for you. Humans comes in different shapes and sizes. Lastly, remember third trimester scans are notorious for being inaccurate. They often over judge by between 15-20%.
Here is a very helpful link to an article on VBAC and big babies:
https://www.thevbaclink.com/get-that-big-baby-out/
9. Will I Need Extra Monitoring?
NICE guidelines recommend continual monitoring for VBAC however this is widely questioned within the independent birthing and midwifery communities.
Wired CTG technology significantly restricts women’s freedom of movement during labour, favours professional authority and undermines a woman’s birthing instinct; it creates inattentive midwives who focus on data instead of women’s bodies and focuses attention on the obstetric bed where the labouring woman is ‘detained’. There is an identified direct correlation between the CTG and an increased caesarean risk and increase of instrumental deliveries (Cochrane Report).
My own position was a steadfast No – unless there was a clear medical reason – for example meconium in early labour and a dipping heart rate.
One of the many reasons women, including myself, opt for HBAC is to alleviate the imposition on the labour of such invasive monitoring.
10. When Should I Decide Whether to VBAC or Go For a Subsequent Caesarean?
Ideally, the sooner, the better. The more time you have to find the best care providers for your VBAC journey, the happier your journey will be.
However, if you are unsure, you can change your mind right up to the 36 week appointment. (I knew one client who changed her mind on the operating theatre, got dressed and went home to go into labour spontaneously).
Whilst you can legally change your mind any time in your pregnancy – the earlier you do it, the more time you have to make good choices and gather a great team around you.
It is better to book an HBAC earlier on and ‘change your mind’ than leave it too late and discover the homebirth team are fully booked.
11. Can I VBAC With More Than One C-Section Birth?
Yes. Although generally two sections plus means a c-section is recommended. However many women have attempted VBAC after a second c-section and succeeded.
12. Should I be Induced if I’m planning a VBAC?
Women aiming for VBAC are expected to have an antenatal clinic appointment for 38-39 weeks where they will have a discussion about postdates management including the options of post-dates induction and post-dates ERCS in place of induction of labour. Cervical sweeps will be offered if appropriate. So be ready for the medicalisation of the end of your pregnancy. Is that what you or your baby need?
A typical induction pathway in the UK for VBAC is:
Mechanical induction of labour using balloon catheter to ripen the cervix over 12 hours followed by artificial rupture of membranes on delivery suite with the option of oxytocin drip if labour does not establish after 4 hours. Low threshold to deliver by emergency caesarean section if any concerns
Here is the NICE guidelines on induction:
The final guideline is:
1.2.19
Advise women that they can choose not to have induction of labour or caesarean birth, even when it may benefit their or their baby’s health [2008, amended 2021]
The risk of scar de-hiscence/rupture is increased two to three fold (2-3:200 labours ) if labour is induced. The risk of c-section is also increased as is the risk of instrumental delivery.
Induction of labour using mechanical methods (amniotomy or Foley catheter) is associated with a lower risk of scar rupture compared with induction using prostaglandins.
Inductions require you to be on a labour ward which undermines the birth physiology and places you back in the clinical model once again with all its potential interventions.
Many inductions are recommended as statistical-based policy rather than necessity. Ask yourself is your baby healthy and well? Do you or your baby really need to end this pregnancy before it naturally completes? You can opt for monitoring instead and refuse or delay induction (see clause 1.2.19 above),.
13. What are my Legal Rights Around VBAC and HBAC?
Woman have a right to receive high quality, evidence-based respectful care in their childbearing year. Women have a right to complete and accurate information to help them make an informed decision about how they want to give birth. Women have a right to give birth without major surgery. Women also have a right to choose their place of birth. (Birthrights)
The hospital is obliged to meet you in your request. If they have a homebirth team which covers your area, they are obliged to support you in your decision to HBAC. The only caveat to that is that they felt you were being dangerous or unsafe. A straightforward VBAC/HBAC does not count as a dangerous birth choice.
14. Why Choose an HBAC?
Homebirth after Caesarean is becoming an increasingly popular and acceptable birth choice.
It appeals to those women who perhaps endured really invasive medicalised labours the previous time and want to do something radically different this time.
Home is where birth is meant to occur; it is where our physiology works best. An uninterrupted labour in the privacy and comfort of your own home is likely to flow much more fluidly than one interrupted by the imposition of labouring in what is essentially a public space.
A study carried out in 2021 found that home-births after caesareans were associated with higher vaginal birth outcomes than planned hospital VBACS.
In choosing home birth, remember you can also choose to transfer in at any time if you decide you need more pain relief or you simply want to be in hospital. It does not work the other way around. You cannot suddenly during labour decide you want to stay at home, if you have not previously booked a home birth.
To find out more about Homebirth visit this great resource:
https://www.sarawickham.com/research-updates/is_home_birth_safe/
15. Should I Return to my Original Health Provider/Hospital?
This is a question regularly raised in podcasts on VBAC.
Here in the UK, you still have a legal right to choose your place of birth and most areas are served by a number of hospitals – all of which have different management systems and teams. So the advice to choose your care provider carefully still stands.
Some hospitals have very vibrant homebirth teams and birth centres, whilst others are regularly closing their birth centres and have scant homebirth teams.
Some hospitals have a much higher c-section rate than others. If your hospital has a high intervention rate and a frequently closed birth centre, it may be time to try a different hospital.
If you are choosing to VBAC, it is important to understand what happened the first time? And why? If your obstetrician recommended c-section last time, why would they not this time? How will future challenges be navigated by the same team? Why would they do something differently?
Obtaining a copy of your birth notes is an essential first task. You may also want to book a debrief with your HCP to go through and make sense of the notes. Or you may prefer to do this with an independent birth professional like an independent midwife, doula or birth-keeper.
First-time parents frequently, and rather naively, place their trust in their HCPS.
Rather than reflecting on whether you should change care provider, interview your care providers properly and ask yourself whether you feel these people really want to support you in your intentions. If there is doubt; move?
These days many UK trusts support HBAC and welcome VBACS into the mid-wife led low intervention birth centres but you have to push for such decisions to be made.
16. How Can I Protect Myself From Coercion at my Appointments?
Your midwife is contractually obliged to book you an appointment with a senior obstetrician because you are a VBAC. They are also contractually obliged to ensure you understand the risks of uterine rupture and maternal morbidity. Finally, they are contractually obliged to assess your likelihood of successful VBAC. That is their job.
Your job is to remember that their lens is limited; that they assess based on their narrow framework of perception. They do not take into account your will, determination, readiness, courage, newfound resilience and the support you intend to gather around you this time. These qualities are not quantifiable. Your job then is to remember that the information the Dr offers to you, you are able to choose whether to accept it – or not. It is an opinion; their opinion. It does not need to be yours. It is certainly not the truth.
17. What do I Need to do to Optimise my Chances of VBAC?
This is the big question. These are my thoughts.
We are all uniquely different versions of the same being. Our differences will require us to need different things; what helps us to feel safe will differ from person to person; but there are a few key pieces of the puzzle that need to be in place to be in place for all of us to ensure we get the best support and outcome on our VBAC journey. These are:
The Best Professional Support
Ensuring your team of HCPs are really VBAC friendly. To VBAC, you need a good midwife more than a consultant. Midwives are the experts in physiological, vaginal birth. A midwife who feel confident working with VBACs is infinitely more valuable than an obstetrician who only knows and see problems. Conversely, there are also some amazing Obstetricians out there as well as midwives who do not trust VBAC. Whilst the NICE guidelines recommend labour and delivery on the delivery suite (Consultant-led unit) as opposed to at home or on the midwife-led birthing unit (MLBU), as I have previously mentioned this is up for negotiation. Remember the guidelines also recommend the support of ‘patient choice’
Interview your care providers properly to find out:
- How many of the women requesting VBAC, get VBAC at their unit?
- How many HBACs complete? How many transfer?
- If you choose to VBAC in hospital, do they offer intermittent monitoring?
- Will they let you in the birth centre?
- Will they allow you access to the pool?
- What is their induction policy for VBACs?
Get a VBAC Doula
I strongly recommend a birth doula with VBAC experience.
Doulas are outside the system so can help you to make informed decisions and advocate for yourself. Doulas will support you in your wishes rather than uphold the guidelines. Doulas will be able to emotionally and physically, if necessary, support you on your journey with massage, guidance and loving care, which the HCPS have no time nor remit to do and, most important, the doula will be able to come to your home and help you to labour at home for as long as possible before you transfer in – ensuring minimal interruptions to birth physiology from the hospital experience. If intervention is recommended, the doula will be able to help you make an informed choice about whether to accept that recommendation – or not.
Debrief Your Previous Birth
This is a biggie. Do not just hope its all gone away and that this will be a different experience. There are many important reasons to debrief the first birth. They include:
Understanding what happened the first time: When I looked at my notes, I saw that my breech labour had been progressing quite well. I was just entering active labour when I agreed to a c-section. My baby was breech and breech births were rare but actually, at that point in time, there was no problem apart from my inability to cope; I was throwing up, crying out in pain; I was suffering.
What I needed in retrospect was someone to look after me; to explain what was happening; to help me adjust to this new intensity; to hug me and to hold me; to show me how to trust the experience. Nobody did that. Instead they recommended c-section every two hours. In the end I accepted what seemed inevitable.
Understanding how you might do things differently this time:
Seeing that gave me resolve; I just needed to learn how to get through the experience; I needed to make it as easy for myself as possible; I needed support, I needed to learn how to turn toward the surges instead of resist them. I chose a homebirth and independent midwives; I practised yoga, and learned everything about being a VBAC. I prepared my body and my mind. I also prepared my baby. We did it together.
Reading my notes was an invaluable experience. As we know many c-sections do not need to occur. Finding out what led to yours is key to you avoiding it the next time.
It is your legal right to access and see you maternity notes: Follow this link to Birthrights for more information on how to retrieve a copy: https://birthrights.org.uk/factsheets/accessing-your-records/#:~:text=You will need to go,the Data Protection Act 2018.
Educate Yourself
Read blogs like this. Listen to the many amazing podcasts episodes on VBAC with wonderful professionals like Hazel Keel . Read the stories of women who VBAC and HBAC on VBAC LINK and vbac.com
Read Hazel Keels book on Birth After Caesarean which is up-to-date and features international research. (Published 2022)
Or Gail Tulley’s Changing Birth on Earth: A Midwife and nurse’s guide to using physiology to avoid another unnecessary cesarean (2020) Gail Tulley is the incredible force behind Spinning Babies.
Do the Inner Work
Only yesterday a homebirth midwife said to me: “Labour is a mind-game. Once you lose your mental equilibrium its game over.”
Mental resistance, fear, doubt and apprehension create physical suffering and pain; you must learn how to face your fears, cultivate trust, practice letting go of control and embrace the experience of surrender.
This is the work of yoga and mindfulness. To find out more about my yoga and mindfulness for pregnancy and birth online course and birth professionals training follow the respective links.
18. What are the Challenges to Successful VBAC?
The other biggie. I have labelled them as C words.
Coercion
Be ready to question recommendations and stand up to coercion – which really kicks in at the end of pregnancy. If I had not refused to be intimated and not ignored recommendations, I would have not have experienced any of any VBACS – because each time there was an ‘issue’. This is why a doula is so important. You need someone who can help you figure out whether you are being coerced or whether this is advice you need to listen to.
Control
Do not let others control your birth. Let your body birth the way it needs to. You do not need to be continuously monitored. You do not need experts telling you what positions to be in or how to labour; your body will do that all by itself – simply listen to your body. You may need to learn how to listen to and trust your body. In a VBAC, your body brings you your baby – not the health professional.
On the subject of control, be ready to surrender your own need to control the physiological experience. This can feel very scary for many. The mind wants to control but birth belongs to the body. A lot of births are sabotaged by control. In order to complete the process, you have to surrender to the immensity of it. This is where yoga and mindfulness come in alongside loving support. These support structures – internal and external – will help you to let go of control when the time is right.
Complications
What stalled the first one? It may arise again. Or new complications may arise – natures curveballs. Like meconium or waters breaking before labour or biomechanical complications. These complications may not lead to the same outcome but can steer you away from your birth plan into new territory. Be informed about possible complications so that should they arise, you have an understanding of your options and are as resourced as possible.
19. What Are The Most Common VBAC Fears
Anecdotally my experience from working with VBAC clients and having many VBAC students in my pregnancy classes, is that VBACS are more worried about un-necessary clinical intervention, induction and malpositioning than scar rupture. Many VBACs also fear their bodies will stall, or their babies will not fit through their pelvis. Often their fears will be based on events from the first birth. Fear is a powerful force so it is important that the inner work of pregnancy includes examining and unpacking fear in all its forms so that you know how to handle fear when it arises.
20. What if my VBAC Fails?
Not everyone who plans a VBAC will succeed in having one. For every 100 women attempting a VBAC, 30-40 will end up with an emergency caesarean.
This is why it is so important to get rid of the language of success and failure; to even attempt a VBAC is to succeed in overcoming fear and trauma; in taking radical responsibility for your body and your birth choice; in choosing to face both the previous experience and your new fear of failure; it is nothing less than a spiritual warriors path.
What we learn about ourselves; our bodies, our babies, the healthcare system and childbirth itself along the way is profoundly meaningful and frequently life-changing.
Reclaiming your body and your birth is already a grand act of love irrespective of the birth journey you get.

Join my VBAC Yoga & Mindfulness Online Intensive (For VBACS and Birth Professionals Supporting VBACS):
on Sunday 12 January 2025.
Listen to my VBAC live with Joy Horner:
Find out More about my Birth Professional Yoga and Mindfulness Training (starts September 2024)
Scholarships available.
Join my weekly online Yoga & Mindfulness for Pregnancy Course