Compulsive catastrophising, the act of regularly imagining the worst possible scenario as outcome, is a cognitive distortion; an unconscious and irrational process that causes great suffering. It is both symptomatic of, and leads to, anxiety, depression, ocd and even post-traumatic stress disorder (PTSD). It is also an implicit maternal policy.
Systemic catastrophising occurs when whole groups collectively magnify potential risks and promote worst possible outcomes without any real proportional evidence. It is always to control. Not only is systemic catastrophising deeply embedded in the collective mind and structure of the maternity services, it has been normalised to the point where the general public no longer see how irrational, unhealthy and dangerous a perspective it is.
At the end of pregnancy, unless your unborn baby sits nicely within a perpetually shrinking definition of normal; as you approach your due date, you will be assigned one (or more) of the following complications; big baby, small baby, advanced maternal age, gestational diabetes, failing placenta, low amniotic fluid, excessive amniotic fluid; Group B Strep; abnormal foetal position, reduced foetal movement, prolonged pregnancy and so on. Inevitably induction will be recommended along with continuous foetal monitoring to assess foetal distress. Statistically speaking the likelihood of further intervention is high. What the maternity service is communicating – even promoting – is that the end of pregnancy is a dangerous time which needs diligent clinical surveillance and intervention to prevent harm to your baby or even stillbirth.
In recent years the implicit campaign to catastrophise the end of pregnancy has been so successful that in 2022 -23, 57 per cent of women cut short their pregnancies with either elective c-sections or inductions. 57%! More than half of all mothers believed their pregnancies were too dangerous to continue. This has never happened in history before.
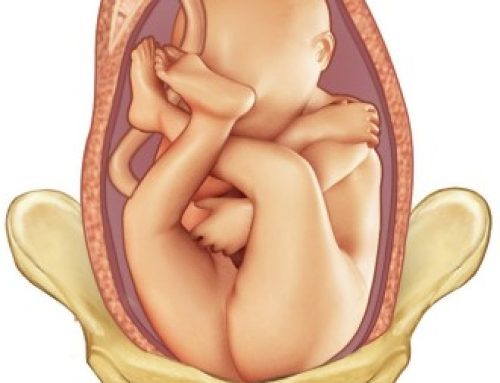
This week, my client was told at 38 weeks that her baby was ‘on the big side’; she was denied access to the birth centre; (her chosen place of birth), and recommended induction at 39 weeks to avoid the risk of shoulder dystocia,( with possible nerve or brain damage to the baby and the additional risks of still birth); third degree tearing and postpartum haemorrhage.
This previously confident and well-prepared mother was suddenly frightened. What happens when you are full of live healthy baby and you hear the words stillbirth? third degree tearing? and post-partum haemorrhage? What are the images that appears in your mind?
Words are like spells used to direct and control the minds of others. Hypnotists, politicians, speech writers, advertisers, lawyers and therapists know this because they regularly engage cognitive biases, emotions, and subconscious thought processes, all the time to shape perceptions and influence decisions. The media regularly amplifies negative narratives which reinforces collective fear.
Statistically speaking, it is equally true that her baby is a healthy size; that her baby will spontaneously initiate labour when he/she is ready to be born; that labour will proceed normally, as most would do if left alone; that the mother will be free of drugs and monitors and will be able to use the pool and move around into a variety of gravity-friendly positions to open her pelvis and birth her baby without instruments or even a graze.
Mothers are educated from the beginning of their pregnancies, through authoritative and directive language, to submit their independence and self-responsibility to the maternity service which assures them they will be looked after and “given the best possible care”.
The Language used is deliberately inclusive and even empathetic but power remains firmly in the camp of the health care provider (HCP) They say things like “lets discuss the best birth plan for your baby,” and” Make sure to call us immediately if there is reduced foetal movement.” And “you’ll need to see the Dr to discuss your birth choices.’ If you stray too far from the care pathway, language becomes more persuasive and directive – designed to deliberately elicit fear: “if you don’t agree to this, your baby could die”. In the birthing community, it’s known as playing the death card and it happened all the time.
How many outlying mothers have heard that well-used statement? I know I have.
Just when you should be nestling into the last days of pregnancy; separating yourself from the drive of industrial life; cooking meals for postpartum and finding a new more horticultural rhythm, you are given a deadline; produce a baby or be induced. Hundreds of thousands of mothers spend the end of their pregnancies in an anxious state attempting to induce their babies naturally with a desperate medley of pineapples, curries, stairclimbing, acupuncture, marathon walks, sex, herbs and castor oil. Partners friends and family worry alongside the mother. Like a virus, fear spreads through the family. The baby now marinading in a daily bath of fear and anxiety. The baby does not come – because, if left alone, on average first time babies gestate beyond 41 weeks. So she packs her bag and takes herself off for an induction. Compliance thorugh fear. Wins every time.
The travesty is that in so many of these cases there was never anything wrong. How many normal healthy pregnancies are pathologized by the paranoid and domineering perspective of obstetrics and its oppressive and defensive medical pathway?
In 2022-2023, 33% of mothers were induced and 40% of babies were born via caesarean section; a further 10% were born via instrumental delivery. The numbers of women experiencing uninterrupted physiological birth is today in the minority – the direct impact of systemic catastrophising is that women are disempowered; they do not trust their bodies and they no longer believe they can give birth without medical assistance. They are frightened of all this intervention, and they are frightened to face birth without it. Women are between a rock and a hard place.
Systemic catastrophising in the maternity services is a toxic force that is removing the normal from birth altogether and transforming it into a clinical process that is completely controlled with little regard for the long term psychospiritual wellbeing of either mother or baby.
What are the consequences of this? According to Birth Better UK, one third of women are experiencing childbirth as traumatic. Excessive pressure and coercion, loss of autonomy, over intervention, the focus on technology over human connection, lack of support, birth injuries from instrumental deliveries; ranging from cuts and infections to pelvic organ prolapse and a life of incontinence and reduced sexual function; as well as an increase in neonatal admissions and inadequate postpartum care; this all leaves a deep physiological and psychological scar. This is the opposite of what reproductive justice stands for; this is an absence of female bodily autonomy and dignity in childbirth.
Dr Michel Odent, former obstetrician and advocate for human physiological birthing believes the loss of female instinct and maternal instinct is one of medicines biggest calamities:“Imagine a mother gorilla giving birth and you trying to take her newborn baby gorilla away from her. Imagine the aggressive, maternal protective instinct that would come up?” Human mothers have the same instinct, but decades of systemic catastrophising and disempowerment through fear have undermined maternal instinct to the point where women have lost their ability to mother from that place.
And what about the baby? What are the consequences for the baby unable to complete its gestation and denied its impulse to initiate its own birth – as nature intends. If the baby is born too early it may have underdeveloped lungs which increases its propensity for respiratory diseases in life; additionally exposure to synthetic hormones and antibiotics affects the baby’s microbiome which is linked to long term poor immunity , induction increases the risk of foetal hypoxia and birth trauma for the baby and if instruments are used to extract the baby, the experience of physical trauma and physical harm is present too. Babies born by elective caesarean are at greater risk of asthma and allergies later in life, and bypassing or interrupting the labour process can seriously compromises the breastfeeding process and can create bonding issues.
In a sane society, says Dr Michel Odent, medical intervention exists to rescue normal birth not dominate it. But our society is clearly not sane.
We should be concerned. For our daughters and their daughters. At this rate the ongoing normalisation of medical birth will erode natural birth practices to the point where they are outlawed altogether; midwifes will become obstetric nurses (they already are) and natural birth advocates will be marginalised. Women will internalise the belief that their bodies are unable to birth without intervention and childbirth, as we once knew it, will be over. This is already happening. Worst case scenario is the intricate and complex process of labour will be bypassed altogether and relegated to the annuls of biological history along with the appendix and our wisdom teeth. This dystopic vision of childbirth is a catastrophic vision I choose not to believe.
Birth belongs to women. Which means women must reclaim it along with tehir bodies and their babies. It is up to mothers, midwives and birthworkers, in all their forms to protect physiological birth and extract us from this collective insanity and expose the systemic catastrophising for the dangerous and harmful practice that it is.
This means a campaign to promote homebirth; and to keep birth centres open; the labour wards should be empty, not the other way around. We need better birth education within the maternity systems, delivered by those outside it, and more psychospiritual support for all on the path to motherhood so that mothers feel mentally strong and ready for labour; not terrified to the point of disempowerment. Finally, we need an independent and accessible watchdog set up to monitor institutional catastrophising and ensure heavy penalties where it is abused.
Reproductive justice is clear: women have the legal right to consent to or refuse any medical treatment during childbirth, even if their decision might result in risks to themselves or their baby.
If the dead baby card is played in your presence. Record the conversation and ask for the evidence. When they say to you the still birth rate doubles after 41 weeks, remind them that what that actually means is the risk of stillbirth rises from 1 in 1000 babies to 1.5-2 in 1000 babies and that you prefer to put your attention on the 999 mothers whose babies were healthy and well at birth.
It is more likely, that your baby does not need rescuing and artificially extracting and that labour can proceed as normal. This is what needs normalising: that childbirth is a straightforward physiological event. Our babies are meant to initiate labour when their gestation is complete. Our bodies bring us our babies when they are ready to be born.
And if you are feeling vulnerable after an appointment, do a reality check. Ask yourself? Is this really true? What’s the evidence? How am I feeling in my body when I believe this perspective? How can I challenge the negativity bias? Write down your fears. Challenge them by listing alternative outcomes and evidence against the worst-case scenario. Seek help if you need help understanding the evidence. Ask for your baby to be monitored if you are feeling vulnerable and unsure.
If you believe your baby is well and you are still catastrophising practice mindful self-awareness to interrupt the catastrophising narrative. This is how to short-circuit and bring an end to catastrophic thinking. Whenever you feel a wave of fear or catastrophic thinking, stop what you are doing, turn fully towards your embodied experience with commitment and concentration to be with the physical experience of fear. Become very present to what you are feeling in your body; put your hands on your belly and really be with the physical felt experience of fear. Notice in what places in your body you feel the energetic expression that we label fear. Is it in your gut? is your heart beating faster? has your throat constricted? How can you tell you are feeling fearful? Breathe slowly and deeply towards the feeling; directly into the experience. You can say to the fear: I see you and I feel you and I accept you. I also choose to believe that in this moment my baby and I are safe. Practice the following heart womb meditation to strengthen your connection with your baby.
Heart Womb Meditation:
Sit in any comfortable position. Become aware of your breathing, no need to change your breathing, simply notice where your body moves as you inhale and where your body moves as you exhale. Bring your left hand to your heart and right hand to baby. Notice the weight and warmth of your hands. Take your awareness down to baby resting in the wombspace. And then back up to the hand resting on your heart. Breathe in to your heart space and as you breath out imagine sending that breath as a rover of light energy down into your womb and the heart of your baby. As you breathing receives that love energy from your baby back into your own heart. Exhale light and awareness from your heart to your baby’s heart. Inhale receiving the light and love of your baby back into yur own. With each cycle of breath exchanging love between the two hearts that reside in your body.
Stay here for as long as you wish.
Then slowly open your eyes.

Other practical tips to manage a fearful state at the end of pregnancy:
Opt to go in and listen to your baby’s heartbeat anytime you need that external reassurance.
Request to see the consultant midwife if the obstetrician is denying you access to the birth centre.
If offered a 36-week scan, it is your right to refuse it. The 36-week scan is not written into policy yet is becoming standard practice across many NHS trusts.
Avoid reading or listening to negative birth stories and out your attention on the kind of birth you do want. Read positive birth stories instead.
Go out into nature every day. We all know how good nature is for mental health.
Express your fears rather than shoulder anxiety alone. Seek out a perinatal counsellor is necessary.
Practice perinatal mindfulness so that you learn how to witness unpleasant emotions with self-awareness and compassion
Connect with your baby through the heart womb meditation daily.
Connect with a group of pregnant women for solidarity and support
Journal all your fears without censor and challenge them by listing alternative outcomes
Invest in your body through pregnancy yoga so that you feel more embodied and connected with it.
Remember catastrophic thinking is a cognitive distortion not a reality. Be diligent about taking on other people’s opinions as truths.
The end of pregnancy is not a time for fear and catastrophising but a time for internal validation and empowerment. By reclaiming our agency and challenging the toxic influence of exaggerated risk narratives, we can foster a healthier mind state, patience and trust in the final days of our pregnancy as we prepare to birth and meet our babies.
References
https://www.aims.org.uk/journal/item/birth-physiology-politics
https://evidencebasedbirth.com/evidence-for-induction-or-c-section-for-big-baby/
https://www.aims.org.uk/journal/item/beware-the-dead-baby-card

Contact Nadia@nadiaraafat.com to find out more about her Yoga & Mindfulness for Pregnancy Online Course (for mothers) and her Birth Doula Service. To find our more about the Yoga & Mindfulness 100 hr prenatal teacher training and 40 hour postnatal teacher training, please click on the hyperlinks.